


Radial Keratotomy or RK is considered to be the grandfather of refractive surgery.
Radial Keratotomy was developed and pioneered in 1974 by a Russian Ophthalmologist named Svyatoslav Fyodorov. It became very popular and often performed in the 80s and early 90s. Although this procedure is no longer performed, millions of Americans underwent this procedure during its “hay day.”
Additionally, further RK treatments and even treatment with other refractive procedures like LASIK were done to undo the damage of Radial Keratotomy. The vast majority of these patients worsened and the severe complications of Radial Keratotomy often even required a corneal transplant called Penetrating Keratoplasty (PKP).
While some patients still retain functional vision, the ill effects of Radial Keratotomy are still being suffered by hundreds of thousands of Americans to this day.
Radial Keratotomy Procedure

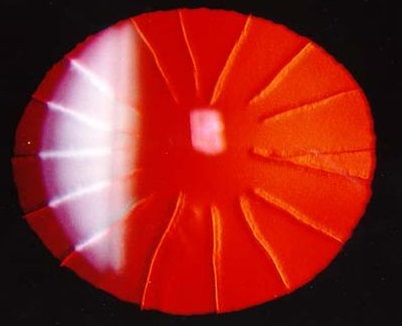
Radial Keratotomy involves making short but very deep cuts in the cornea. There are various levels of correction depending the on the severity of nearsightedness. Anywhere from 4 to 32 radial cuts were made in the cornea to correct nearsightedness as well tangential cuts (called AK) to correct for astigmatism. These cuts relax and flatten the cornea to compensate for nearsightedness.
The problem with Radial Keratotomy is that it never stops progressing!!
Complications of Radial Keratotomy
At the time, surgeons did not understand the stability or refractive effects that these cuts would have years and decades down the line.
The cuts from Radial Keratotomy weaken the bio-mechanical strength of the cornea. As a result of these changes, the cuts never stop flattening the cornea. While many Radial Keratotomy patients enjoyed successful outcomes initially, studies show 40-50% of RK patients continued to progress. This results in FAR overshooting the intended prescription and often developing very high and very irregular hyperopia and astigmatism.
Imagine if the corneal surface was the like the shifting sands of a desert.
In addition to flattening, the destabilizing cuts also cause the cornea to change shape… often. Wildly fluctuating prescriptions are very common. The severity of the prescription changes correspond with the number of incisions made in the cornea. These changes in prescription can occur month to month or year to year. This makes determining the prescription a moving target for eye care providers and makes glasses and traditional contact lenses ineffective and very frustrating.
Additional mechanical risks are possible simply because of the deep cornea incisions. These incisions often never completely heal. As a result, there is always the risk of corneal rupture after trauma, like a bad fall or a car accident. Also, these cuts can become infected or small areas around the cuts can slough off and cause a painful corneal erosion.
How to correct vision after Radial Keratotomy
 Since the cornea is constantly changing like shifting sand, the goal of refractive treatment is to create a new, more stable front surface of the eye. This is achieved through hard, specialty contact lenses. Hard contact lenses cover over the irregular and variable corneal surface and provide stable and consistent vision.
Since the cornea is constantly changing like shifting sand, the goal of refractive treatment is to create a new, more stable front surface of the eye. This is achieved through hard, specialty contact lenses. Hard contact lenses cover over the irregular and variable corneal surface and provide stable and consistent vision.
Small diameter hard lenses are usually not very useful because the cornea after Radial Keratotomy is incredibly flat. Small lenses on a very flat surface have difficultly gaining purchase and tend to slide off the cornea.
As a result, the main therapy is very large diameter lenses called Scleral Contact Lenses. Despite their large size, Scleral Contact Lenses are very comfortable compared to small hard lenses and well tolerated.
Newer Refractive Surgeries
 Modern refractive surgery, such as LASIK and PRK, are usually safe and very effective ways of reducing the need for glasses and contact lenses. Any reputable surgical center will screen you for risk factors that might portend corneal problems months or years down the line. Additionally, longer term studies on LASIK also seem to suggest that this procedure will not have the unintended and devastating complications of Radial Keratotomy.
Modern refractive surgery, such as LASIK and PRK, are usually safe and very effective ways of reducing the need for glasses and contact lenses. Any reputable surgical center will screen you for risk factors that might portend corneal problems months or years down the line. Additionally, longer term studies on LASIK also seem to suggest that this procedure will not have the unintended and devastating complications of Radial Keratotomy.
Occasionally, the corneal strength of the cornea can be weakened by modern refractive surgeries like LASIK. This corneal compromise doesn’t cause flattening or prescription fluctuations like with Radial Keratotomy. Instead, it causes the cornea to lose its structural integrity and bulge outward.
This is called refractive ectasia, ectasia meaning irregular bulging of the cornea. Ectasia can occur if early Keratoconus (especially Forme Fruste KCN) is missed during the preoperative evaluation or can simply be a result of the procedure itself.
If refractive ectasia is developed, glasses and contact lenses will not properly correction vision because of the irregular bulging surface. In this case, as well, specialty hard contact lenses will improve vision and quality of life.
We have seen many, many individuals with severe visual complications of refractive surgery.
In nearly every case we have been able to VASTLY improve vision and quality of life with Specialty Contact Lenses.
If you are unsatisfied with the outcome of your surgical procedure. Consider scheduling a evaluation at our facility.
Additional Links about Radial Keratotomy and Refractive Ectasia: