Statistics and Associations
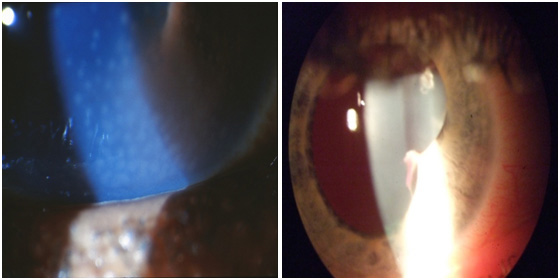
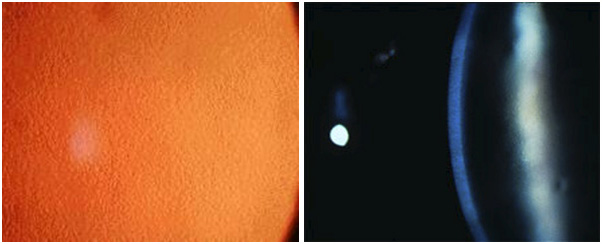
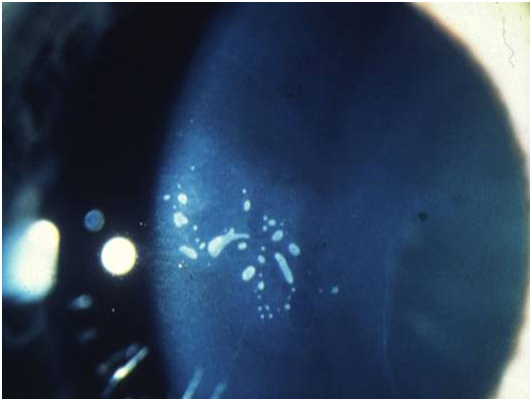
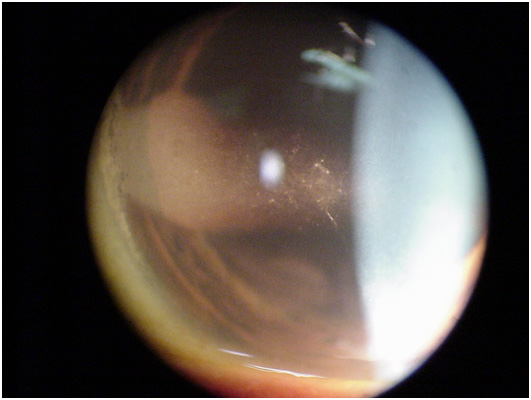
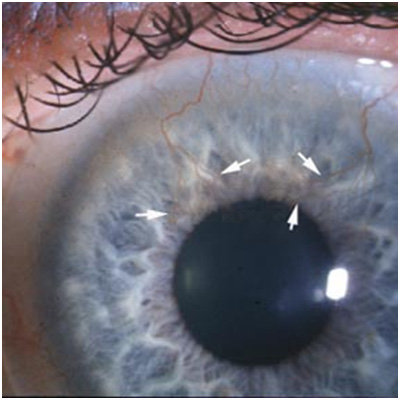
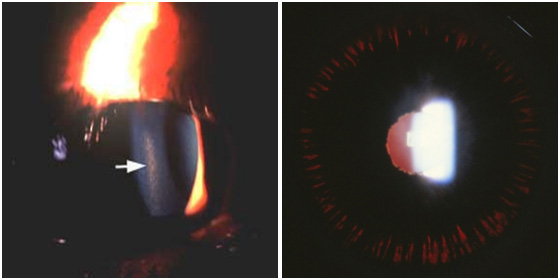
- Liberation of iris pigment cells into anterior chamber can clog drainage canal and increase pressure
- Typically first seen in white males between 20–40 years old
- Visual fluctuations common with physical exertion
- Pigmentary glaucoma occurs in approximately 10-20% of patients
- If glaucomatous changes occur from PDS, usually happen before fifth decade of life
Management
- No treatment recommended unless glaucomatous changes occur
- Laser treatments quite effective as well as topical medications